A pinched nerve is one of those phrases that gets used loosely. People say it for anything from a quick twinge in the neck to genuine, persistent numbness in the hand. Most cases that come into our office and get called “pinched nerve” actually are real nerve compression, and once you know what the pattern looks like, it’s pretty easy to recognize.
This post covers what’s actually happening, where it most commonly shows up, what makes it worse, and what to do about it.
What a Pinched Nerve Actually Is
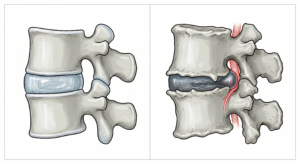
Nerves run from the spine out to every part of the body. They pass through small openings between vertebrae and travel through narrow channels surrounded by muscle and connective tissue. A “pinched nerve” is what happens when one of those passageways narrows enough to put pressure on the nerve.
The compression can come from a few sources:
- A bulging or herniated disc pressing on the nerve root
- Bone spurs (osteoarthritis-related) narrowing the foramen the nerve passes through
- Tight muscle compressing a peripheral nerve as it travels
- Inflammation around the nerve from injury or repetitive strain
- Postural compression from sustained bad positioning
The compressed nerve sends garbled signals to the part of the body it serves. That’s why pinched nerves cause symptoms not just at the spot of the pinch, but down the path of the nerve.
How to Tell If You Have a Pinched Nerve
Before you read through the pattern below, here’s a quick explainer on telling pinched nerve from shoulder pain:
Pinched nerves have a distinct symptom pattern. If you have most of these, it’s a strong candidate:
- Pain that radiates down an arm or down a leg, not just localized to the neck or back
- Numbness or tingling in a specific region (a hand, a foot, an outer thigh)
- Burning or electric quality to the pain, not just a dull ache
- A specific position that triggers or relieves it (turning the head, reaching overhead, leaning back)
- Weakness in the muscles served by that nerve, in more advanced cases
Pain that’s just localized stiffness or general soreness is usually not a pinched nerve. It’s muscle or joint pain. Pinched nerves announce themselves by traveling.
Where Pinched Nerves Most Often Show Up
Cervical nerves (C5 to T1). These exit the lower neck and supply the shoulders, arms, and hands. Compression here causes radiating arm pain, hand numbness, and weakness. Triggers include sustained forward head posture (see Tech Neck), sleeping wrong, or whiplash injuries.
Lumbar nerves (L4 to S1). These exit the low back and supply the buttocks, legs, and feet. The most well-known pinched-nerve case is sciatica, where the L4, L5, or S1 nerve roots are compressed, causing pain down the back of the leg. We have a dedicated guide on sciatica for that pattern specifically.
Peripheral nerves (away from the spine). Carpal tunnel (median nerve at the wrist), cubital tunnel (ulnar nerve at the elbow), and tarsal tunnel (tibial nerve at the ankle) are all peripheral pinched nerves. These are common in patients with repetitive hand work or specific anatomical setups.
The pattern of symptoms tells us which nerve. The location of pain and numbness maps to a specific nerve’s territory, which is why a careful history and physical exam usually identifies the source without imaging.
Common Causes
For most patients, the pinched nerve isn’t a random event. It’s the result of a pattern that built up over time.
Posture-driven cases. Forward head posture and rounded shoulders gradually narrow the spaces in the cervical spine where nerves exit. Eventually a small extra load (sleeping odd, a long drive) is enough to tip into actual nerve compression.
Disc-related cases. Discs degenerate or bulge with age and repetitive load. When a bulge or herniation pushes into the foraminal space, the nerve gets compressed. These can happen suddenly (lifting something wrong) or gradually.
Injury-driven cases. Whiplash from a car accident, sports impacts, and falls all can cause acute nerve compression by injuring the structures around the nerve.
Repetitive use. Carpal tunnel in office workers, cubital tunnel in patients who lean on their elbows, ulnar nerve compression in cyclists. The repetitive position gradually inflames the tissue around the nerve.
How Chiropractic Care Treats Pinched Nerves
The right treatment depends on which nerve and what’s compressing it, but a few core tools work across most cases:
Chiropractic adjustments. Restoring proper motion to the joints around the compressed nerve usually decompresses the space the nerve passes through. For cervical and lumbar nerve roots, this is the primary intervention.
Soft tissue work. For peripheral nerve compressions (carpal tunnel, piriformis syndrome), manual release of the muscles compressing the nerve is often the highest-leverage move.
Dry needling. When the surrounding muscles are chronically tight and compressing the nerve, dry needling releases the muscle directly. This is especially effective for cervical radiculopathy and piriformis-driven sciatica.
Postural and ergonomic correction. If the cause is sustained bad positioning, we’ll work out what’s driving the position and adjust the desk setup, sleep position, or activity pattern.
Specific home exercises. Nerve gliding exercises and targeted stretches help mobilize the nerve through its sheath, which speeds recovery.
Most patients see meaningful improvement within 2 to 6 weeks of consistent care. Acute cases often respond faster. Chronic cases (months or years of symptoms) take longer because the surrounding tissue has had time to adapt to the compression.
When NOT to Wait
A few presentations need urgent attention rather than a routine appointment:
- Sudden, severe weakness in an arm or leg (drop foot, inability to grip)
- Loss of bladder or bowel control (this is an emergency, go to the ER)
- Saddle anesthesia (numbness in the area that would touch a saddle)
- Pinched nerve symptoms after a fall, accident, or head injury within the last 24 hours
- Pain that’s getting rapidly worse over hours, not days
These can indicate more serious nerve injury that may need imaging or surgical evaluation. Don’t wait on these.
Frequently Asked Questions
Will a pinched nerve heal on its own?
Some mild cases will, especially if the underlying cause is removed (sleeping position, work setup). But many won’t, and the longer the nerve is compressed, the higher the chance of chronic symptoms even after the pinch is relieved. Earlier treatment generally means faster recovery.
Do I need an MRI?
Usually no. Pinched nerves are mostly a clinical diagnosis from history and physical exam. We order imaging when symptoms are severe, when there’s significant weakness, or when standard treatment isn’t producing the expected response.
Can chiropractic adjustment make a pinched nerve worse?
Done correctly, no. We’re not forcing motion against a compressed nerve. We’re restoring motion to the joints around it, which opens the space. Our pre-treatment exam identifies any presentation where adjustment isn’t the right first move.
Should I use ice or heat?
For acute, sharp pain: ice for 15 to 20 minutes a few times a day in the first 48 to 72 hours. For chronic muscle tightness contributing to compression: heat. Most patients with pinched nerves do better with ice early, then heat once the acute pain backs off.
What about cortisone injections?
Cortisone can provide short-term relief by reducing inflammation around the nerve, but it doesn’t fix the underlying compression. We generally recommend trying conservative care first and reserving injections for cases that don’t respond.
Can a pinched nerve come back?
Yes, if the underlying cause isn’t addressed. The patients who fix their pinched nerves and don’t have them recur are the ones who also fix the posture, ergonomics, or movement pattern that caused it.
Get Started
If you’re dealing with radiating pain, numbness, or tingling, we can help figure out what nerve is involved and get you on a treatment plan that addresses both the symptom and the cause.
We see patients from West Omaha, Millard, Elkhorn, and the broader Omaha area.
Book your visit online or call (402) 330-8600.
Related: Disc Health: How to Keep Your Spinal Discs Healthy for Decades — pinched nerves often start with disc issues; this guide covers prevention.
About the Author
Dr. Dane Becker found chiropractic the way a lot of his patients do: through pain. A weightlifting injury in college left him with such intense back and chest pain he thought he was having a heart attack. His trainer sent him to a local chiropractor, the pain backed off almost immediately, and he was hooked.
Since 2008 he’s been practicing in West Omaha, serving patients from Millard, Elkhorn, and the broader Omaha area. He’s trained in sports injuries through postgraduate CCSP education and a specialist in whiplash and auto injury cases. He’s worked with numerous NFL, NBA, and MLB players, plus college and pro female athletes. Becker Chiropractic & Acupuncture is a multi-year Best of Omaha winner. When he’s not at the clinic, he’s with his three kids (Colson and twins Lyla and Liam), and the family is happiest on a beach.


{kind=link}